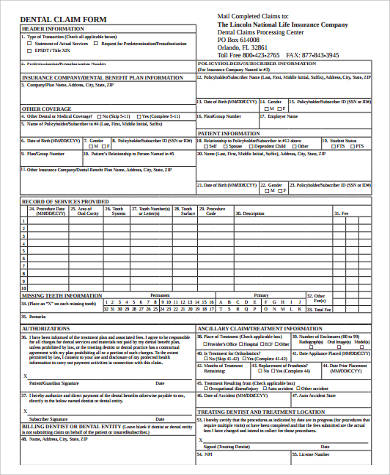
manhattan life dental claim form
VB Health Screening Benefit. Box 925309 Houston TX 77292-5309 Customer Service.
![]()
Manhattan Life Health Insurance Plans
Many may ask that you pay your share of the cost at the time of the visit.
. Dental Vision and Hearing insurance from ManhattanLife is designed to meet as many needs outside of standard medical insurance as possible. Enter your details to begin. 247 patient benefit verification claims and remittance statements.
By registering and logging in I acknowledge and agree to be bound by the Terms and Conditions for this web site. Report a Death Claim Online Form Acknowledgement of Misplaced Policy. Coverage you can count on.
Beneficiary Claimant Statement - Under 5000. ManhattanLife VB Claims PO Box 926169 Houston TX 77292 Customer Care. Lookup Policy Note that TaxID date of birth.
Or contact our Customer Service department. Show your ManhattanLife Assurance. Select the appropriate form category below.
Visit the ContractPolicy Holder website to submit it online or use the Easy Upload mobile app for iOS and Android and. Manhattan Life has been insuring Americans for over 170 years. Signature If Claim Is For A Minor Parent Or Legal Guardian Must Sign Date Submit Completed Form to.
Lookup benefits without registering or logging in. Follow these simple steps to get THE MANHATTAN LIFE INSURANCE COMPANY Claim Form ready for sending. Coverage you can count on.
Or contact our Customer Service department. As one of the longest. Signature If Claim Is For A Minor Parent Or Legal Guardian Must Sign Date.
Dental Claim Form The UFT Welfare Fund Dental Claim Form is used for two different. Open the document in. Ad Download Or Email Form JY0333 More Fillable Forms Register and Subscribe Now.
ManhattanLife Assurance Company of America 10777 Northwest Freeway Houston Texas 77092 DENTAL VISION HEARING CLAIM FORM 800-669-9030 Claimants Proof of Loss. Dental Vision and Hearing insurance from ManhattanLife is designed to meet as many needs outside of standard medical insurance as possible. VB Accident Claim Form.
Claim for dental vision and hearing expense benefits. Many ophthalmologists and optometrists will file the claim on your behalf. 247 patient benefit verification claims and remittance statements.
1-800-669-9030 Annuity Contract Owners. This is a Limited Beneift Insurance Policy for Dental. Life Health Policyholders.
Signature Printed Name. Standard ADA dental claim forms will also be accepted by the Administrator. Select the form you want in our library of templates.
One Huntington Quadrangle Suite 1S03 Melville New York 11747 1-800-520-3368 Fax 1-516-887. Box 926169 Houston TX 77092 Mail to the following. VB Accident Claim Form.
Please choose the appropriate form below. VB Assignment of Benefits. For more information contact Careington at 800 290-0523.

Lyner9nh9njn M
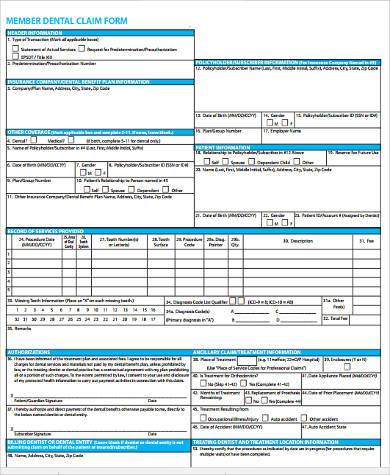
Free 9 Sample Dental Claim Forms In Pdf Ms Word

Manhattan Life Dental Steven Insurance Agency Anguilla Ms
Free 9 Sample Dental Claim Forms In Pdf Ms Word

Illinois Individual Dental Plans
![]()
Dental Vision And Hearing Insurance Dvh Manhattanlife

Manhattanlife Client Services

Western United Life Medicare Supplement Tidewater Management Group

Dental Vision And Hearing For Seniors Manhattanlife
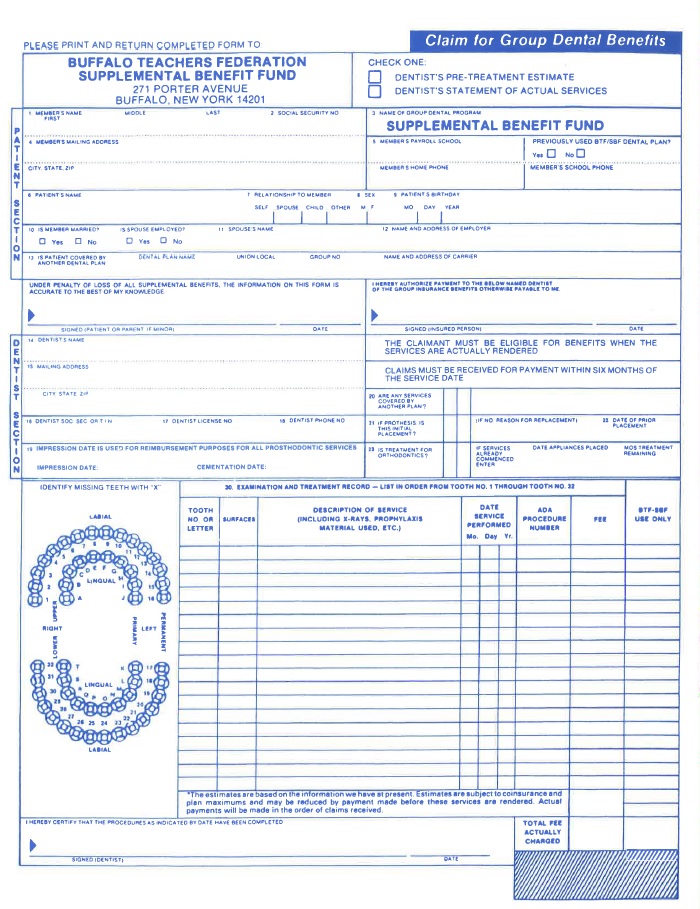
Buffalo Teachers Federation

Standard Ada Form Fill Online Printable Fillable Blank Pdffiller
![]()
Dental Vision And Hearing Insurance Dvh Manhattanlife

Manhattan Life Medicare Supplement Plans For 2022 Medicarefaq

Dental Vision And Hearing Insurance Senior Benefits Of Georgia

Manhattan Life Dental Need Dental Insurance The Best Dental By Expert Insurance Team Medium
![]()
Manhattanlife Medicare Supplement Plans Medigap Insurance In 2022
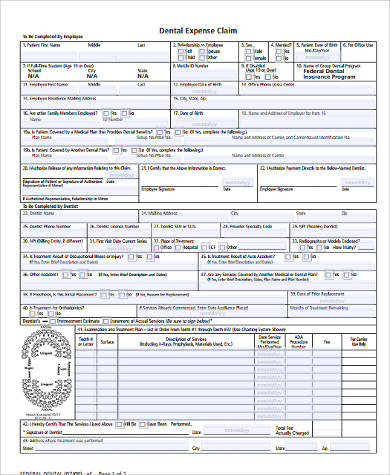
Free 8 Dental Claim Forms Samples In Ms Word Pdf

Dental Vision Hearing Ppt Download

Get Appointed With Manhattanlife Insurance Company New Horizons Insurance Marketing Inc